Three Things To Read This Week
1. Report: Here’s What It Takes To Launch A Crisis Stabilization Center.
In a new report published by Policy Research Associates, researchers examined jurisdictions planning and operating centers, then compared findings on service capacity, staffing, funding, partnerships, evaluation, and implementation challenges to get one of the clearest pictures to date of what it takes to launch and operate a successful Crisis Stabilization Center. Researchers found that these centers are workable, increasingly common, and worth the effort—especially when jurisdictions plan deliberately, braid funding streams for stability, and build strong partnerships across public safety infrastructure—concluding that “the costs of establishing and maintaining a CSU… [are] worth the investment.” The full 20-page report is worth your time, but here are some of the toplines:
Works In Communities Of All Sizes—With A Variety Of Crisis Services: The survey shows crisis stabilization centers are not limited to large cities—among the sites studied, “72% serve an area with a population of 500,000 or less,” while only “6% serve an area with more than 1.5 million.” Most are community-based programs that offer a range of crisis services, including “voluntary (with walk-in) capacity,” the ability to “provide minor medical clearance… transportation services… sobering and/or detox services,” as well as “formal discharge planning,” and follow-up care. Operational models are flexible as well: “Sixty-nine percent … offer services with a length of stay of 23 hours or less,” while “49%… have programs with LOS greater than 23 hours,” “25% offer programs with LOS of 7 days or longer,” and “10%… have LOS of 30 days or longer.”
Short-Term Stabilization Leads To Better Outcomes Than Jails Or ERs: Researchers found that these facilities “provide short-term stabilization and treatment for individuals experiencing a behavioral health crisis in a setting that is less restrictive than a hospital or jail.” Many operate as rapid-stabilization hubs: “69% of the centers offer services with a length of stay of 23 hours or less,” while “90% are open 24/7” and “85% have voluntary (with walk-in) capacity” to stabilize people quickly, avoid unnecessary emergency department use or incarceration, and connect individuals to “ongoing treatment and community-based services.”
The Most Successful Centers Are Highly Collaborative Across Existing Health And Law Enforcement Infrastructure: The researchers found that “almost all crisis centers collaborate with hospitals/emergency departments (97%) and law enforcement (95%).” Most also partner with “local community providers such as mental health or substance use providers (92%), EMS (87%), and mobile crisis teams (83%).” These partnerships extend further into the community ecosystem, including “housing providers and shelters (67%), fire departments (65%), and county behavioral health agencies (68%).”
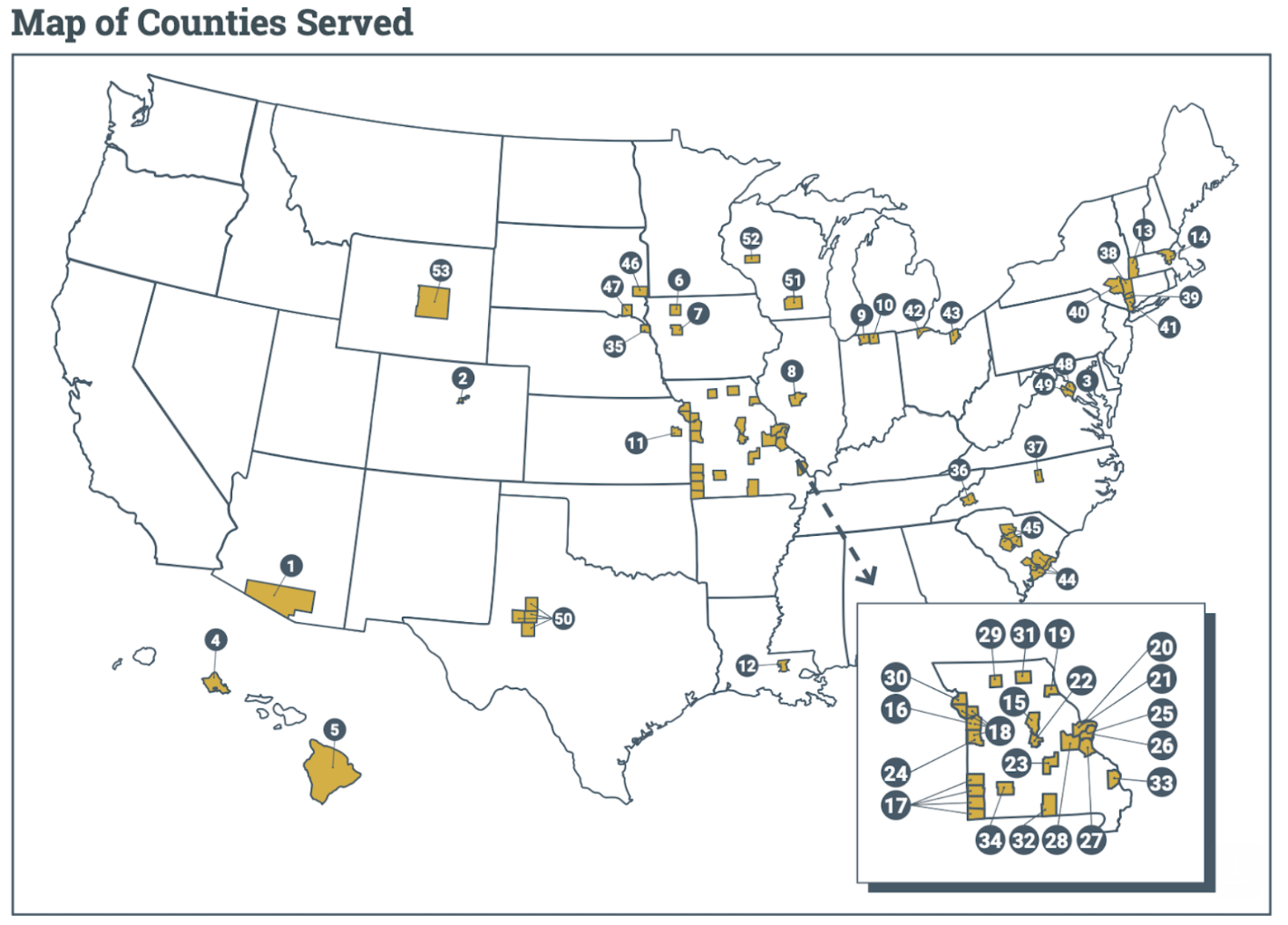
Here’s a map of the various facilities that participated in the research:
Momentum For Crisis Stabilization Centers Opening Around The Country:
In Buffalo, New York, New Crisis Stabilization Center Serves Nearly 200 Patients In First Month Of Operation. For WGRZ, Lauren Hall reports on the region’s new crisis stabilization center—“the first facility of its kind in Western New York”—that just opened its doors last month and already served “more than 175 people in mental health crisis.” The facility provides an alternative model to jails and emergency rooms for people experiencing acute cases of “anxiety, depression, substance use, or any other mental health crisis … [and allows] patients [to] stay for up to [24 hours], though most are stabilized within four to five hours.” Trained medical professionals at the facility provide “emotional and behavioral support … medication support… support for mild to moderate withdrawal or intoxication… [and] psychosocial assessments” to patients immediately when they arrive.
Paige Hawkins, who oversees clinic services at the facility, explained to the news station that the high volume reflects both that the facility is such a stark difference to a jail or emergency room setting—it’s “a very calm environment and … it is welcoming, that the staff are welcoming.” She added that patients are coming in saying they have “never had this level of care because unfortunately up until now the system didn't allow for it.”Clark County, Nevada Opens Doors To “First Crisis Stabilization Center” In The County, Designed To “Ease The Strain On Hospital Emergency Departments And The Justice System.” For Hoodline, Olivia Rivera reports on the historic new center—a partnership between the county and University Medical Center—“a 24/7 outpatient facility in North Las Vegas for adults experiencing acute behavioral health emergencies… [that] takes walk-ins and allows fast drop-offs from law enforcement and emergency medical services, to offer a calmer, home-like setting instead of a busy ER or a holding cell.” The 17,000-square-foot-facility is “staffed around the clock by licensed mental health professionals and nurses… providing psychiatric evaluations, medication support, medically assisted therapies and brief, solution-focused interventions… [and] is built to stabilize most patients within hours, then link them to follow-up services.” Mason Van Houweling, the ceo of the medical center that houses the crisis stabilization facility, explained to the news site that “the goal for most patients is ‘less than 24 hours’ … a quicker cycle meant to free up hospital and law enforcement resources while getting people connected to ongoing care.”

Bernalillo County, New Mexico Crisis Stabilization Center Celebrates Two-Year Anniversary: “We Are The Safety Net.” For University of New Mexico Sciences News, Tamara Lopez reports on the center’s milestone—a partnership launched by UNM Hospital and Bernalillo County—that has transformed the public safety infrastructure in the region, having “helped many people find the right care for themselves and their loved ones… ensuring those in psychiatric crisis have a safe place to go so that behavioral health professionals can assess next steps.” Dr. Mauricio Tohen, professor and department chair of Psychiatry and Behavioral Sciences, explained to the news site that two-fold feature of the facility have allowed the medical professionals on staff to provide treatment to the most patients: the crisis triage center, which “provides medium-acuity crisis stabilization for adult patients… [where] patients can stay for up to two weeks if they need to.” And the peer living room—a “space that offers low-acuity and walk-in services to patients… for people to get connected with services they need… [and is] open to people 18 years old and older, and it’s staffed by peer experts … who are trained to offer support who also have first-hand experience with mental health conditions and the challenges that come with navigating them.”

2. Cities Look To Transit Safety Ambassadors To “Provide… And Enhance… Safety And Security.”
Albany, New York, Launches First Transit Ambassador Program. The Capital District Transportation Authority announced the launch of the first-of-its-kind team in the region last month. The team, designed to ease strain on law enforcement resources, provides a highly visible layer of safety experts, who are already present “on select routes and will rotate throughout [the] route network… an approachable, visible resource focused on assistance and engagement.” The trained ambassadors “serve as a visible and positive presence on our buses… helping customers navigate the system, supporting our operators, and … serve as a connection to community resources … ensuring our riders and employees feel supported every day.”

Kansas City Announces Expansion Of Transit Ambassador Team, Increasing Staff By More Than 300 Percent. For KCUR, Jodi Fortino reports on the city’s massive expansion of the transit ambassador team, as part of an $80 million overhaul of the city’s public safety infrastructure in anticipation of the World Cup arriving this Summer. The team, which the city is hoping to expand by 50-60 ambassadors, outfitted in highly-visible blue uniforms and vests, are a “welcoming, knowledgeable and calming” presence “across the transit network… [as they] assist passengers… de-escalate tense situations, and… [are trained in] “CPR and Narcan administration.” Staff Terri Barr-Moore, chief of staff for the city’s transit system where the ambassadors are housed, explained the team’s expansion simply: “They provide … [and] enhance… safety and security…"

3. Mobile Crisis Response Teams Expanding Around The Country, Reducing “Hospital Visits And Law Enforcement” Involvement.
North Carolina Launches Mobile Crisis Response Teams, And “High-Tech” Mental Health Dispatch, Pilot Aimed At “Freeing Up Law Enforcement Resources” And “Speeding Response,” Across The State. For Queen City News, Bailey Striepling reports on the new pilot, part of a statewide effort from Gov. Josh Stein to strengthen the state’s mental health system, that establishes “a real-time dispatch process that streamlines response to individuals in crisis wherever they are… [and] will get people directly into mental health care with a mobile response team, freeing up law enforcement.” The pilot is designed to “function like a high-tech 9-1-1 for mental health, sending mobile crisis teams directly to a caller’s location” and is expected to be “operational in 27 North Carolina counties by the end of April, with the ultimate goal of expanding it statewide.”

Maine Mobile Crisis Response Team Has Responded To More Than 3,400 Mental Health-Related Calls For Service. WGME reporting on the milestone, writes “In 2025 alone [mobile crisis response teams] supported more than 3,400 interventions, serving communities from Androscoggin County to northern Cumberland County… offering immediate, on-site mental health support for children and adults in distress.” The teams, composed of trained mental health professionals, arrive on scene and immediately begin “conducting risk evaluations… performing mental status exams to determine a person’s psychological state; and [deploying] de-escalation techniques.” They can “travel to homes, schools, and community locations... to stabilize individuals in the moment and connect them to longer-term care options” and help reduce “hospital visits or law enforcement [involvement].”
Lane County, Oregon Brings Youth Mobile Crisis Team In-House, Making Responder Team Full County Staffers, Similar To Fire, EMS And Law Enforcement. For LookOut, Ben Botkin reports on the county’s historic move away from third-party providers to staff the mobile crisis team, and instead, bring the mobile crisis team in-house, to make them county-level staffers. Lane County “has been providing mental health services to children and adolescents for over 50 years,” NBC News reported, and the mobile crisis component has been a recent and successful advancement of that effort, expanding the team with “responders specifically trained to serve youth through mobile crisis response.” The 24/7 teams provide “services for youth up to age 18, and coordinates with the county’s mobile crisis service program for adults to decide which cases to take for youth who are up to 20 years old… handled 2,659 calls for children and youth in crisis” in just 2025.
