Three Things To Read This Week
1. Study: “Consistent, Long-Term Engagement” In Hospital-Based Violence Intervention Programs “Can Cut Future Violence In Half.”
Boston Medical Center along with the Health Alliance For Violence Intervention held a briefing this week about a “landmark” new study published last month in the Annals of Internal Medicine, from researchers at Boston University that found “a 50% reduction in violent injury or involvement in violent crime for participants of the Violence Intervention Advocacy Program, or VIAP, at Boston Medical Center… findings marking a significant milestone about the life-changing impact of hospital-based violence intervention programs nationwide.”
Jonathan Jay, the lead researcher on the study as well as a professor at BU’s School of Public Health, explained to The Brink, BU’s magazine covering its latest research, that he and his research team “analyzed the records of 1,300-plus shooting or stabbing survivors, ages 16 to 34, who were at high risk of violence… almost half of them worked with VIAP sometime in the first month after their discharge, and the researchers found that brief interaction did not appreciably lessen the risk of future violence when compared with patients who never used the program. But the roughly 10 percent of survivors who regularly worked with VIAP in the first two months after discharge saw their likelihood of being involved in violence cut in half.”

Jay added that this is “the most important project I’ve ever worked on” because the findings could help other cities model effective hospital-based violence intervention programs after the success of Boston Medical Center’s program. The Brink’s Rich Barlow details how the program works:
“For survivors of gunshot and knife wounds treated in the emergency department, VIAP provides post-discharge help with mental health and family support services and assistance, if necessary, with connections to housing, food, employment, education, and other needs….
Currently, when someone is admitted to the hospital with a violent penetrating injury, they meet with VIAP patient advocates during their stay or soon after. Those advocates build relationships and conduct needs assessments to help target issues—from safety planning to mental health to housing insecurity—that could slow recovery or increase potential involvement in future violence … The mental health support is given in collaboration with BMC’s Community Violence Response Team.
VIAP differs from other intervention programs [across the country]... in its unusually robust services—it has 13 staffers. Although the study focused on young adults, VIAP is more flexible than many other programs … in its availability to violence victims outside of the highest-risk groups and in letting participants decide how often to avail themselves of its services.”
Jay explained that “People who get shot or stabbed are vastly more likely to have been excluded from systems—kicked out of school, kicked out of housing, to have some history of criminal legal system involvement so that it’s harder for them to get a job… [but as the VIAP data demonstrates] when people’s basic social and emotional needs are met, they are far less likely to be involved in violence…”
Related: In a recent two-year study from UCLA’s Luskin School of Public Affairs, researchers examined the impact of the Newark Community Street Team—one of the country’s most prominent community violence intervention programs—to determine whether NCST’s model of community-based violence interruption works and whether it is scalable for other cities looking to launch or enhance their CVI offerings. The researchers concluded that NCST’s model “provides rigorous evidence that community-led violence intervention can significantly reduce violent crime” and “offers a scalable blueprint” for cities around the country. The full 200-page report and executive summary are worth your time, but here are some of the topline findings:
Intervention Teams Deploy At The Same Time The Threat Of Violence Rises: Researchers found a “significant moderate correlation between high risk interventions and violent crime at lag 0,” indicating that NCST interventionists are deployed “simultaneously with violent incidents rather than operating on a delayed response model.” The analysis shows the program is “reactive and responding to an immediate need,” validating NCST’s strategy of “responding to, intervening in, and mediating community conflicts in real-time.”
Resources Were Directed To The Communities With The Most Violence: Ward-level analysis confirms NCST directs resources to the neighborhoods most affected by violence—the South and West Wards, where violent crime rates are “approximately 2.5 times the national average,” receive the most concentrated programming. Researchers write the analysis “affirms NCST’s strategy of allocating resources to neighborhoods experiencing the highest burden of community violence” and reflects the program’s “decade-long evolution from pilot project to established practice.”
Program Expansion And Community Engagement Growing: The study documents significant growth in the program’s activity and reach—“high risk interventions doubled between 2022 and 2023,” while participation in the Public Safety Round Table increased “from 2,207 participants in 2022 to 2,560 in 2023.” Researchers conclude this reflects “increased community engagement” and shows NCST is “building a generally more robust infrastructure” while continuing to “expand programming and outreach.”

2. Report: National Standards For Building The Workforce Behind America’s Modern Crisis Response Systems.
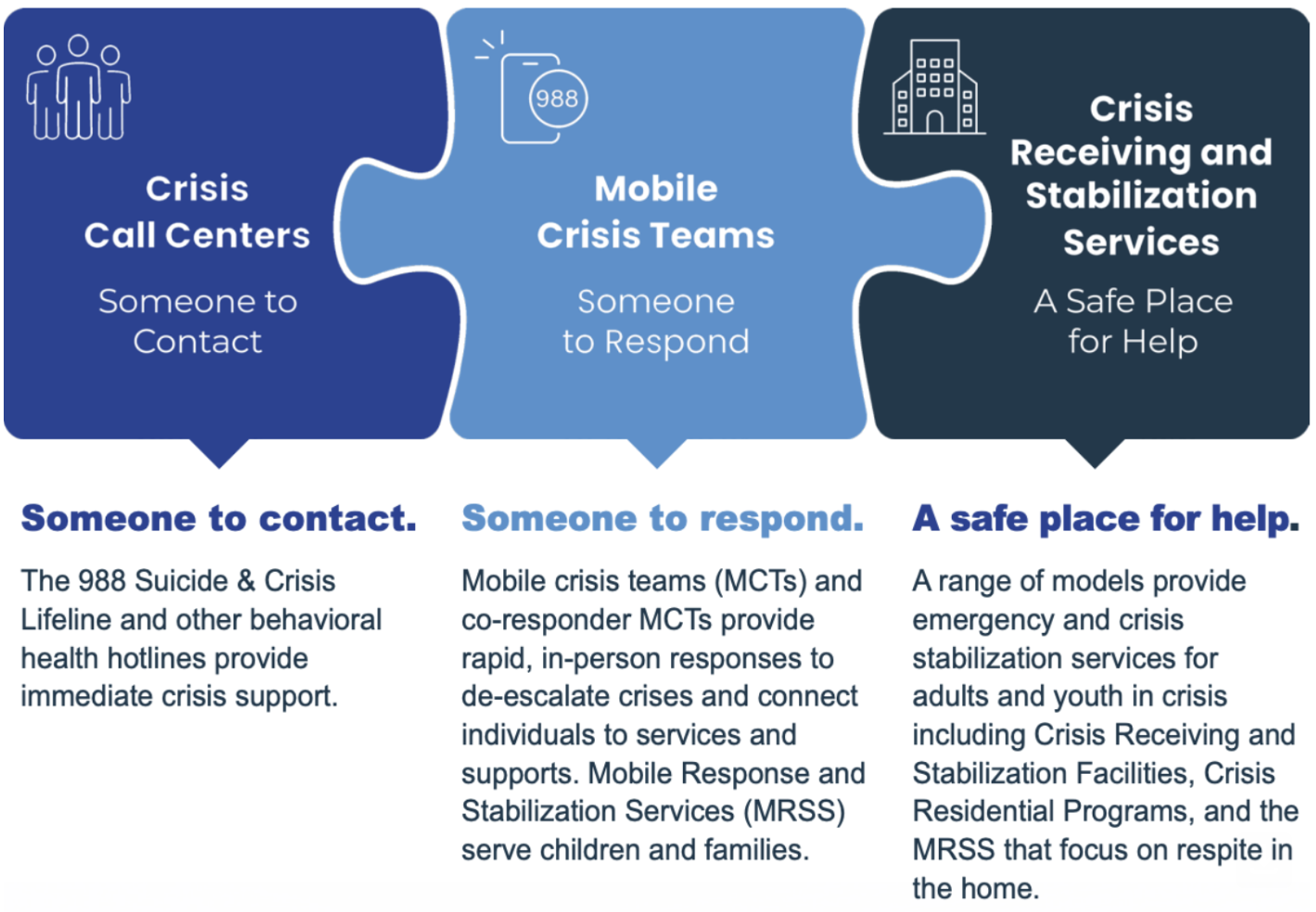
In a new advisory published by the U.S. Substance Abuse and Mental Health Services Administration (SAMHSA), researchers and federal policy experts outline national model standards for crisis care workers as more cities, counties, and states are building out behavioral health crisis systems. Researchers conclude that workforce shortages remain the “largest barrier to providing crisis care services around the country” and argue that new credentialing standards can help “build a skilled, representative, and billable workforce with the capacity to meet demand across the continuum.” Here are some of the key findings from the report:
Workforce Shortages Are Limiting Expansion Of Crisis Systems: The report warns the biggest constraint on crisis systems is workforce capacity, noting that “workforce shortages are the largest barrier to providing behavioral health crisis services 24/7 statewide” across the country. Nationwide, the shortage is severe: “122 million people in the United States lived in a Mental Health Professional Shortage area,” a number “approximately equal to one third of the population.” Rural communities are especially affected because they “have fewer providers per capita than urban areas.”
A New Workforce Model Is Needed: Crisis systems depend on a wide range of responders “providing care across the crisis continuum,” including “social workers, licensed behavioral health workers, therapists, and certified peer specialists.” Because these roles have “different education and training standards … and provide differing levels of care,” the advisory argues that states should establish shared standards so crisis systems can function as an integrated workforce.
Training And Credentialing Systems Are Key To Scaling Crisis Response: The advisory argues that formal training pathways are essential to scale crisis care, recommending national standards covering “core values, competencies, education and training requirements, certification, credentialing, supervision, and ethical standards.” These standards are intended to help states create crisis provider credentials and “build a skilled, representative, and billable workforce with the capacity to meet demand across the continuum,” enabling crisis care to be available “to anyone, anywhere, at any time.”
Related: SAMHSA’s report follows a recent study, published in Psychiatric Services journal, that also found that the rapid expansion of mobile crisis response programs is outpacing the behavioral health workforce needed to run them. Researchers explained that the growth of this “third branch of public safety,” alongside police and fire, has been “hampered by limitations of the behavioral health workforce.” Nationwide shortages remain significant, with 34 states reporting gaps in mobile crisis staffing, particularly among “social workers and other licensed providers, peers, and bilingual staff.” To address the gap, the authors proposed creating a new professional role with “distinct values, competencies, and skills,” that expands on SAMHSA’s recommendations, including:
Establishing a new frontline role—the “community behavioral health crisis responder.” The field needs “a new professional role… rooted in unique competencies rather than attached to existing advanced academic credentials,” allowing systems to recruit and train responders specifically for crisis work rather than relying solely on traditional clinical professions.
Establishing statewide crisis workforce credentials. Researchers urge states to formalize the field through certification programs, recommending that “state behavioral health agencies as well as independent state and national credentialing agencies should establish and manage a credential.” Some states are already developing these certifications, helping define the skills, competencies, and standards for crisis responders
To scale the workforce and meet the demand, researchers recommend expanding training infrastructure—particularly through community colleges, which are “well positioned to prepare trainees for credentialing” and can serve as “a pipeline for the local crisis response workforce.” The report also proposes regional “centers of excellence” to provide training, standards, and technical assistance for crisis response workforce development.
3. Momentum For Mobile Crisis Response Programs Around The Country.
Ithaca, New York Launches New Crisis Responder Team For Mental Health Calls For Service, That “Aims To Reduce Reliance On Traditional Policing When A Law Enforcement Response Is Not Appropriate.” Finger Lakes News reports on the new three-year pilot of a mobile crisis response team, called Responders Offering Outreach, Trust, and Support, or ROOTS, that will respond to some mental health and behavioral health calls for service. City leaders explained that the new responder team will be “integrated… into [core] first response systems [to] ensure that all calls for service can receive the most appropriate response,” and can be “dispatched through 911, requested by the Ithaca Police Department, or self-engage” when they see a person in crisis, ensuring that people “receive immediate support… and remain connected to social services.”
The goal of the team is to operate as a third branch of public safety in the city, and is aimed at “reduc[ing] reliance on traditional policing when a law enforcement response is not appropriate” and “working alongside traditional policing… the mental health responder team, and other [homeless] outreach programs across the city.”Los Angeles City Council “Makes Permanent Its Unarmed Crisis-Response Pilot Program, Diverting [Mental Health] Emergency Calls … Away From The Los Angeles Police Department To Specialized Clinicians.” My News LA reports on LA City Council’s unanimous approval to make the city’s mobile crisis response team “permanent” and “establish a centralized dispatch system that aims to improve response to emergency calls by sending out appropriate teams” for the various crises that enter the emergency response system. This is the first step toward “consolidating all unarmed crisis response initiatives into a single, citywide program… [which include] well-being checks… homelessness… mental and/or behavioral crisis, conflicts that could be resolved through mediation… [so that when] residents call 911 dispatchers, [they] can then divert calls to a centralized center” which then sends the right responder team to the crisis.
The establishment of the team as a permanent branch of the city’s public safety infrastructure follows a successful pilot, that city leaders called a “resounding success,” and saw the team respond to “more than 17,000 calls for service with over 96% resolved without police involvement,” since the team first launched in 2024. City leaders also highlighted that the program also saves taxpayer dollars, explaining that it “costs taxpayers roughly $85 per hour to deploy LAPD officers [to mental health-related calls], whereas the same response from a specialized unarmed crisis response team costs approximately $35 per hour.”
Council President Marqueece Harris-Dawson explained to the newspaper that “The data is incontrovertible and unassailable… we’ve done the work now… the two can exist side-by-side, and when appropriate, either [police or mobile crisis response] can show up” to a crisis depending on the need.

Columbus, Ohio, “Shifting More 911 Responses From Police To Clinicians.” For The Columbus Dispatch, Jordan Laird reports on Columbus Mayor Andrew Ginther, and the City Council, announcing an expansion of the city’s mobile crisis response team, following a successful pilot, “shifting more 911 responses from police to clinicians,” and now the team will “respond to calls without police escorts for the first time.” The mobile crisis response team, which launched in 2024, has responded to “23,000 calls, or about 10% to 20% of all appropriate calls due to limited hours and scope.” Mayor Ginther, a champion for the team, explained to the newspaper, that “every emergency circumstance requires trained expert attention,” with some emergencies requiring a police officer, like robberies or homicides, while other crises, like mental health calls for service, require different expertise: “when an emergency involves an individual experiencing trauma, or mental health or addiction crisis, a trained clinician is best positioned to help… when someone needs stabilization and ongoing support, they should get a pathway to services, not a stay in a jail cell.”