Three Things To Read This Week
1. Momentum For Crisis Stabilization Centers Around The Country.
New Crisis Center In Memphis Provides Patients Mental Health Care, “Rather Than Booking Them In Jail Or Taking Them To Local Hospitals.” For The Daily Memphian, Aisling Mäki reports on Binghampton, Tennessee’s new $34 million crisis stabilization center that is reshaping how the city responds to mental health emergencies, providing “people suffering [with] mental health crises access [to] appropriate care, rather than booking them in jail or taking them to local hospitals.”
The 55,000 square foot facility houses a trained staff of 120 “psychiatrists, nurse practitioners, registered nurses, peer support specialists, counselors and social workers” who provide patients with access to “immediate crisis care… including crisis stabilization and outpatient care for adults experiencing severe psychiatric distress [including] post-traumatic stress disorder, depression or severe anxiety” as well as “behavioral health treatment [and] … detox treatment.” To help both facilitate care to patients and to get first responders back into the community as quickly as possible, county first responders—from mobile crisis response teams, to law enforcement, to paramedics—have “a dedicated drop-off area with key card access to expedite crisis admissions.” The center is open 24 hours a day, seven days a week, 365 days a year” and is free of charge and regardless of health insurance status.

Roanoke, Virginia Opens “First-Of-Its-Kind” Crisis Stabilization Center, To “Reduce Burden On Law Enforcement Officers.” The Roanoke Times reports on the opening of the Blue Ridge Behavioral Health Care Center which provides “access to mental health and substance use care and an alternative to [emergency rooms and jails] with 24 hours a day, seven days a week service.” For Fox News in Roanoke, Zoe Mowery detailed that the facility is staffed with trained mental health experts—including therapists, psychiatrists, nurses, and others—who help patients with “emergency care, residential stabilization [care], crisis intervention ... and outpatient treatment.”
Allison Taylor, the Division Director of access to care for the Blue Ridge Center, explained to the news station that the goal for the center is to operate like an emergency room does for physical wound care, but instead Blue Ridge is focused on mental health care. The facility can handle longer term care needs as well as fast-moving emergencies from “walk-ins, ambulance, fire and police drop offs” so “anyone can access the care” inside the facility: “We think about this as our sort of crisis campus[,] meaning that all of our crisis programming is located in this one space.”

The facility is part of Virginia’s Marcus Alert system, a new state law that “requires that trained [mental health] professionals respond to mental health calls,” rather than law enforcement, in order “to keep people in crisis—due to a mental illness, substance use disorder or intellectual and developmental disabilities—from being arrested and booked in jail.”
The Center is also part of the first round of a $58 million statewide investment, spearheaded by Governor Glenn Youngkin, called “Right Help, Right Now” that “invests in building emergency room alternatives to care for patients experiencing a behavioral health crisis.” Virginia's secretary of health and human resources, John Littel, explained during the announcement of the new investments that these crisis stabilization centers are a critical component of the state’s public safety infrastructure, “ensuring same-day care for individuals experiencing a behavioral health crisis” as well as “reduc[ing] the burden on law enforcement officers.”
2. New Poll: Voters Strongly Believe That Crisis Stabilization Centers Make Communities Safer.
To gauge public support for Crisis Stabilization Centers as a public safety strategy, Safer Cities recently conducted a national survey of 2,414 registered voters.
We defined Crisis Stabilization Centers as “specialized facilities designed to provide immediate support to individuals experiencing acute mental health or substance use crises.” We also explained that “each center is staffed with trained mental health professionals, provides a short-term place to stay while the person stabilizes, and connects the person with longer-term care options.”
Then, we asked: “How effective do you think crisis stabilization centers are as a method of making your community safer?”
Here are the results:
89% Of Voters Say Crisis Stabilization Centers Are “Effective” At “Making Your Community Safer.”
By an 82-point margin—89% to 7%—voters view crisis stabilization centers as “effective” as opposed to “not effective.”
These results also reflect broad bipartisan support, including 94% of Democrats and 88% of Republicans who say crisis stabilization centers are effective.

The Most Convincing Arguments In Favor Of Crisis Stabilization Centers. We then provided participants with “a few statements about the effectiveness of crisis stabilization centers” and asked them to tell us “how convincing, if at all” each of those reasons are “for implementing crisis stabilization centers as a public safety policy?” Here are the three most persuasive arguments:
+84 Net Effective (92% to 8%): “Emergency rooms cannot serve as a backstop for a broken mental health system. Crisis stabilization centers ease the burden on overcrowded emergency rooms that need the space to treat heart attacks, gunshot wounds, and burst appendixes.”
+82 Net Effective (91% to 9%): “Jails are not ideal locations to provide mental health care. Thus, people with mental illness frequently cycle through jail over and over again because their underlying mental illness persists. Crisis stabilization centers break this cycle by addressing acute mental health needs and connecting the person to longer-term care. How convincing, if at all, do you find this as a reason to invest in crisis stabilization centers?”
+74 Net Effective (87% to 13%): “Crisis stabilization centers ease the burden on overcrowded jails, which is important because overcrowding creates a dangerous environment for both the guards who work in jails and the people who are confined in them. How convincing, if at all, do you find this as a reason to invest in crisis stabilization centers?”
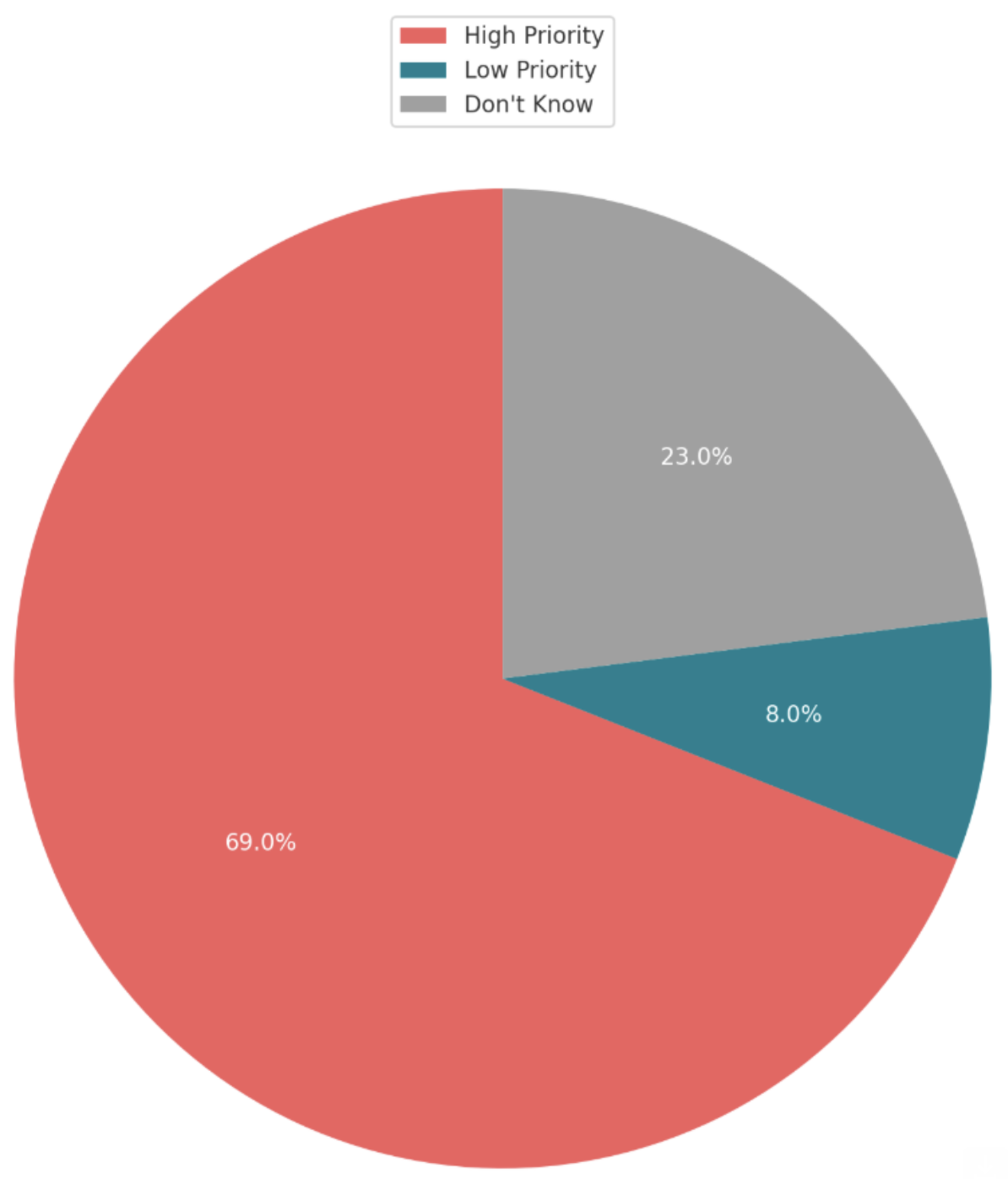
69% Of Voters Say Local Leaders Should Make Crisis Stabilization Centers A “High Priority” In Their Public Safety Budgets. After participants heard arguments for and against crisis stabilization centers, we explained that “local governments often balance many competing priorities and very tight public safety budgets.” We then asked: “Given these budget constraints, how should your local city council or county commission prioritize crisis stabilization centers?”
By a 61-point margin—69% to 8%—voters say local leaders should make crisis stabilization centers a “high priority” in their public safety budgets.
These results also reflect bipartisan majorities, including 80% of Democrats and 63% of Republicans who say local leaders should make crisis stabilization centers a “high priority” in their public safety budgets.
When Forced To Choose, Voters Strongly Prefer To Allocate New Public Safety Dollars To Crisis Stabilization Centers Than On Building New Jails. Read question wording here.
82% = “Spend the additional funds on specialized care facilities such as crisis stabilization centers.”
9% = “Spend the additional funds to build new jails.”

82% Of Voters Support The Creation Of Crisis Stabilization Centers Where They Live. After exposing participants to a variety of arguments in favor of crisis stabilization centers, an equal number of arguments in opposition to spending more money on these programs, as well as questions about prioritization around budget, we asked respondents: “Knowing what you know now about crisis stabilization centers, would you support or oppose the creation of a crisis stabilization center in the community where you live?”
By a 77-point margin—82% to 5%—voters say they “support” the creation of crisis stabilization centers where they live.
These results also reflect broad bipartisan support, including 89% of Democrats and 76% of Republicans who say they “support” the creation of crisis stabilization centers where they live.

3. NEW RESEARCH: “Crisis Receiving and Stabilization Facilities: Designing Systems for High-Acuity Populations.”
Dr. Margaret Balfour, a professor of psychiatry at University of Arizona and a “national leader in crisis care,” is out with a new paper on how policymakers can construct the most effective Crisis Stabilization Centers in their communities.
Dr. Balfour argues that for these centers to be as effective as possible, they need to be designed from the beginning around both “customer needs which include individuals and families in crisis,” who will be receiving care at the facilities, as well as “key community stakeholders like first responders” who will be taking people in crisis to the facilities.
Here are some of Dr. Balfour’s key design strategies to make crisis stabilization a more effective alternative to jails and emergency departments:
“Receiving centers must be quicker and easier for law enforcement to use compared to arresting and booking a patient into jail.” As Dr. Balfour notes, while cities across the country are launching mobile crisis response teams, and other non-police first responder units, to handle mental health and drug overdose crisis calls, “the default first responder has historically been law enforcement rather than emergency medical services. This makes law enforcement a particularly important customer because they are also the first point of entry into the criminal legal system and have a choice between taking the person to jail versus a healthcare facility.”
A “No Wrong Door” policy—ensuring first responders can always drop off individuals in crisis, no questions asked. Balfour explains: “Police officers are not clinicians and cannot be expected to make complex triage decisions regarding which crisis facility to take someone. When officers are turned away, they are discouraged from attempting [to drop off] in the future. Therefore, the crisis center must receive individuals 24/7 with a ‘no wrong door’ policy. If an individual arrives who may need services at another program or facility the person or first responder is not turned away. Rather the crisis facility staff evaluates the person, stabilizes, and arranges for a referral or transfer if needed.”
“Medical stability” not “medical clearance”—allowing direct access to crisis care without requiring an unnecessary emergency room visit. Balfour explains that “The American Association for Emergency Psychiatry, an organization composed of both psychiatrists and emergency medicine physicians, recommends a shift away from the vague and unhelpful [practice of] ‘medical clearance’” which requires a “visit in the [Emergency Department] prior to arrival at the crisis facility… undermining the goal of avoiding unnecessary ED visits.” Balfour argues, physicians at crisis stabilization centers can instead perform “a medical evaluation to determine whether the patient is medically stable for treatment in a crisis facility… ie, the behavioral health symptoms are not likely due to a medical condition, and ongoing treatment for any co-occurring medical conditions is within the scope of the crisis facility.”
Emergency Rooms and Jails Are “Ill-Equipped To Treat People With Behavioral Health Conditions.” Balfour explains that local leaders across the country have constituents “with high acuity symptoms and behaviors [who] warrant special attention when designing crisis systems… [and that] this population can be the most challenging to serve, but also is the greatest in need of specialized crisis care.” When cities “lack facilities that can accommodate these needs, jails and [Emergency Departments] are often the only remaining options… [which] are ill-equipped to treat people with behavioral health conditions.” Here’s why:
Emergency Rooms regularly handle behavioral health emergencies, they often lack the specialized resources needed for effective psychiatric care, as Balfour details:
“46% of EDs lack psychiatric consultation.”
“59% of EDs must transfer psychiatric patients elsewhere due to lack of resources.”
In jails around the country, “about two in five people who are incarcerated have a history of mental illness” which is “twice the prevalence of mental illness within the overall adult population” and has exacerbated the “significant lack of access to adequate mental health care” often found in jails and prisons, as the National Alliance on Mental Illness reports:
“About three in five people with a history of mental illness do not receive mental health treatment while incarcerated.”
“More than 50% of individuals who were taking medication for mental health conditions at admission did not continue to receive their medication.”