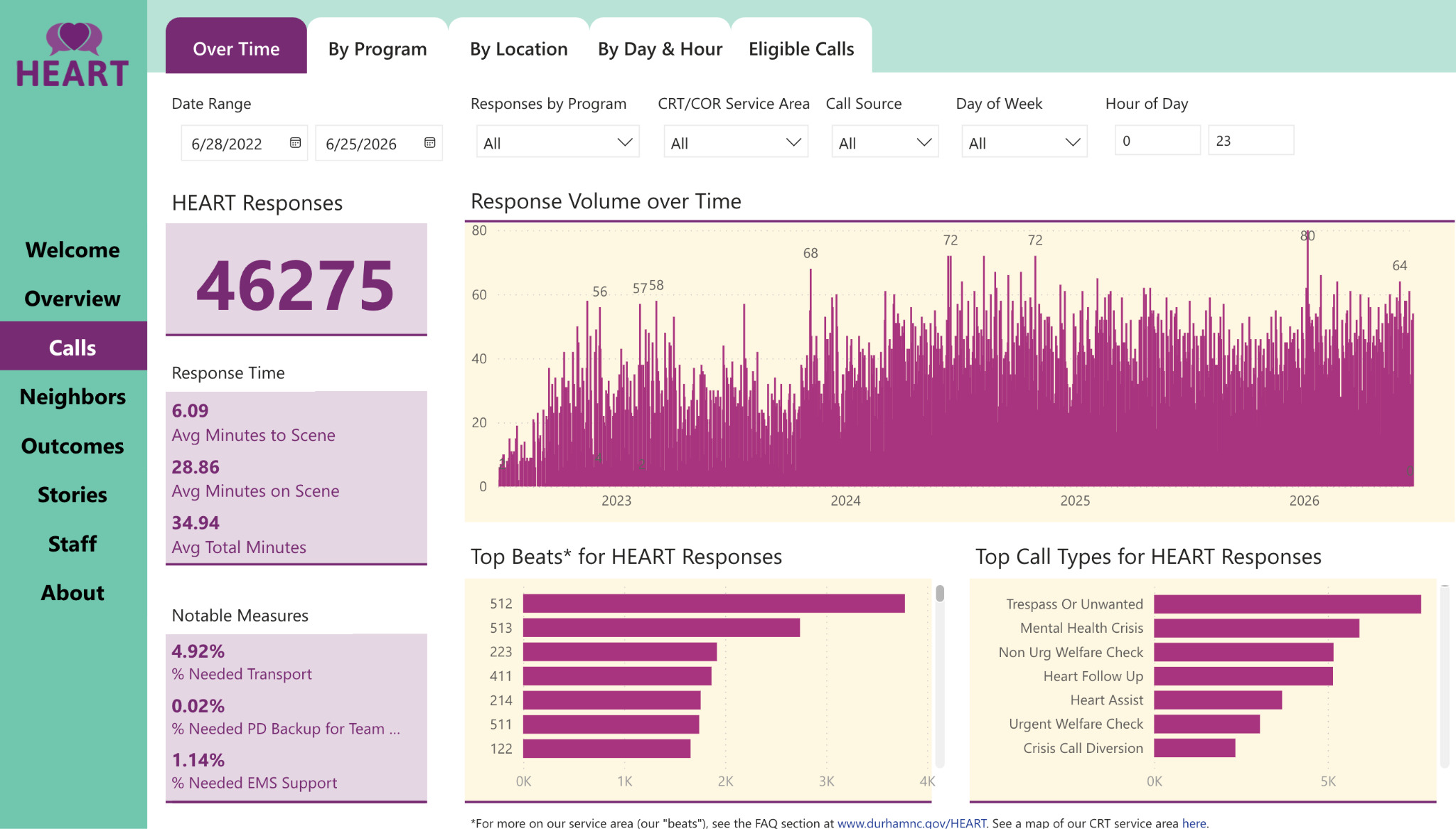
1. Study: Durham HEART Eases Strain On Law Enforcement, Increases Public Safety, And Is “A Good Investment For The City.” A new report published by research institute RTI International examined Durham, North Carolina’s Holistic Empathetic Assistance Response, or HEART, program— a widely watched mobile crisis response model funded by the City of Durham and operated by the city’s Community Safety Department. As Safer Cities recently reported, HEART hit a major milestone this year, having responded to more than 45,000 emergency calls since its launch and has “helped avert thousands of crises and alleviated a strain on the police department.” For this evaluation, researchers analyzed HEART’s first three years in operation, drawing on data from HEART, Durham 911 dispatch, and Durham Police Department records, and using a quasi-experimental design to compare HEART-eligible calls handled by HEART with similar calls handled by patrol when HEART was unavailable.
Researchers found Durham’s model is delivering on exactly what many cities hope to achieve with mobile crisis response teams: reducing strain on law enforcement while improving outcomes for people experiencing mental health crises. Researchers conclude that deploying trained “community responders … to 911 calls instead of law enforcement is associated with fewer enforcement-related outcomes,” the researchers write, including “significantly lower rates of offense reports, arrests, and citations relative to patrol-only responses.” The full report is worth your time, but here are some toplines:
- Reduces Strain On Law Enforcement. RTI found that crisis response team “deployment is associated with significantly lower enforcement actions compared with patrol-only responses for comparable eligible calls,” with the “clearest incident-level outcome differences” showing “a meaningful reduction in arrests and, to a lesser extent, citations.” Researchers conclude that these findings represent “one of the clearest incident-level outcome differences observed” for HEART, showing that the model can reduce unnecessary enforcement while safely resolving eligible calls.
- Matches The Right Responder To The Emergency. Rather than relying on a single team, HEART routes calls to three different response models: a clinician embedded in the 911 center for crisis call diversion, an unarmed community response team for many behavioral health calls, and a clinician-police co-response team for higher-risk situations. Over the study period, “nearly three-quarters of all HEART responses were handled by the teams alone.” Staff documentation also showed service connection, not just call clearance: “93.7% recorded service events resulted in successful contact and engagement,” and in “97% of instances, staff reported the right response was sent.”
- Returns On Public Safety Investments. Researchers found “limited differences in response time compared to patrol,” while crisis response teams spent “on average, only 5 minutes more on scene” as they connected residents to care and coordinated services. Combined with “significantly lower enforcement actions” and an average additional cost of “about $14 more across all call events,” the report concludes HEART “has been a good investment for the city.”
Three More Cities Turning To Mobile Crisis Response Teams To Enhance Public Safety:
- Nevada’s First Mobile Crisis Team Launches In Henderson. For KSNV News, Marie Mortera reports that Henderson has launched the state’s first program to dispatch licensed clinicians directly to people in crisis through 988. The two-person teams will communicate with dispatch by radio, “meet with the individual and gather information,” and “talk to other people in the scene who have information.” Clinical Supervisor Lisa Kelso said the goal is to “meet people where they’re at, with this mental health crisis,” while also “free[ing] up our law enforcement resources so they can respond to more law enforcement calls.”
- “Mental health Crisis Response Program Launches In Rochester,” New York. ABC13 News in Rochester reports the launch of HOPE First, a new peer-led crisis response program serving two Rochester neighborhoods. Program Director Halima Aweis said, “What we know with certainty is that when someone is in crisis, what they need is … someone who has been there, someone who understands.” In addition to mental health emergencies, the HOPE First team will respond to substance use calls, wellness checks, youth crises, elder concerns and other emergencies “without involving police” in order to free up law enforcement resources.
- Solano County, California, Expands Mobile Crisis Response Team Countywide. The Daily Republic reports that the Solano County Board of Supervisors approved an agreement with the California Department of Health Care Services to continue expanding the county’s mobile behavioral health crisis response program using a $1 million state Crisis Care Mobile Units grant. County officials said the funding will support “mobile crisis readiness and service expansion in all cities throughout the county” through crisis vehicles, dispatch staffing, program coordination, training, outreach, and technology and data infrastructure.
2. Safer Cities Interview With Houston Recovery’s Sobering Center. Sobering Centers give people who are intoxicated a place to sober up until they are not a danger to themselves or others. They also provide a safe place to receive medically-assisted detox, mental health treatment, peer support and aftercare.
One of the nation’s longest-running examples is the Houston Recovery Center, whose sobering center opened in 2013 as just the second of its kind in Texas. Open 24 hours a day, the center accepts referrals from law enforcement, hospitals, emergency departments and community settings, where clients receive care from emergency medical technicians, behavioral health professionals and state-certified peer recovery specialists. The center says being staffed by peers makes the difference in helping keep “a bad night from becoming a worse night” while diverting thousands of people from jail and connecting those who need it instead to ongoing recovery resources.
Safer Cities recently spoke with Suzanne Jarvis, Director of Strategic Initiatives at the Houston Recovery Center, about how sobering centers strengthen public safety systems, what makes Houston’s model unique, and why more communities are looking to these programs as an alternative to jail and emergency departments for people experiencing intoxication.

- On Addressing What Jails And Emergency Rooms Are Not Designed To Solve: “HRC sobering center was created to address the following issues: Divert individuals from jail, directing them to behavioral health services without a criminal charge, reduce the jail population, freeing resources for more serious crimes, preserve law enforcement resources, returning understaffed officers faster to the street, provide a chance for many to escape the revolving door of substance abuse and incarceration, shifting from punishing offenses to treating their root cause, [and] preserve medical resources, bearing enormous costs from intoxication visits.
The problem sobering centers address is one that neither jails nor emergency departments are designed to solve: problematic substance use and intoxication, which can create health and safety risks for individuals and the community.
Sobering centers provide an appropriate destination for individuals experiencing intoxication. They serve as a missing doorway to care within a recovery continuum of services focused on prevention, intervention, stabilization, treatment, and long-term recovery maintenance.”
- On Establishing Clear Protocols To Match Each Person To The Right Level Of Care: “Safe admissions are guided by policies and protocols that establish eligibility criteria, assessment procedures, and monitoring requirements throughout a client’s stay.
Houston Recovery Center admits individuals who meet the following criteria: they must be at least 18 years old, ambulatory and able to safely get in and out of floor-level cots, behaviorally stable enough to remain safely in an open dormitory environment, and meet established medical and vital sign parameters set by the medical director.
Throughout the stay, clients are monitored in accordance with established clinical and operational protocols to ensure their safety and identify any changes in medical or behavioral status that may require transfer to a higher level of care.”
- On Building Trust: “Stigma remains one of the most significant barriers to individuals seeking help for substance use disorders… Houston Recovery Center was founded on recovery-oriented principles of compassion, dignity, and respect.
Our frontline team includes Certified Peer Recovery Support Specialists who bring firsthand understanding of the challenges and opportunities associated with recovery. This shared experience helps foster authentic connections with clients and creates an environment where individuals feel understood rather than judged.
Establishing trust is often the first step toward recovery and can increase a person’s willingness to consider treatment, recovery support services, and other life changes… Our doors remain open 24/7. Clients can return whenever they need assistance, whether the next day, the following month, or years later.”
3. Toolkit: Harvard Helps Cities Measure What Matters Most In Alternative Crisis Response. A new toolkit from the Harvard Kennedy School Government Performance Lab gives city leaders a practical roadmap for measuring how alternative response programs are reaching eligible 911 calls, resolving incidents, connecting residents to services and making decisions around investment in programs. The three-part toolkit is built around a practical reality many cities encounter as alternative response programs grow: “key information is spread across systems, defined differently in 911 computer-aided dispatch (CAD) software and alternative response records management systems (RMS), or not captured at all.” Rather than asking cities to start from scratch, the toolkit helps programs “use existing data systems to generate clear, reliable, and accurate metrics” and build “a shared data language spoken across jurisdictions” — giving leaders a stronger foundation for managing programs, showing impact and making the case for continued investment. Here are some key findings from the toolkit’s three reports—data dictionary, guide for calculating metrics, and a FAQ for troubleshooting common data challenges:
- Identify And Track Demand. Harvard recommends that programs track “eligible 911 incidents” — meaning “the number of 911 incidents deemed eligible for the alternative response team, regardless of whether the alternative response team responded or was available to respond.” The FAQ says this metric can “inform strategic discussions on program iteration, sustainability, and growth,” and recommends programs track “alternative response eligibility and ineligibility for all [emergency] incidents … regardless of whether the alternative response team responded.”
- Capture What Happens Once A Call Comes In. The toolkit recommends collecting “two data points — incident disposition and encounter outcome — for each 911 incident to describe the outcome of the response.” Incident dispositions “describe how the program operates as a first responder in the 911 system,” while encounter outcomes show “whether the team engaged with the individual in crisis” and capture “the needs of and services delivered to the individual in crisis.” The Data Dictionary defines “engaged and offered services” to include when a team “provides a referral, voluntary transportation, and other services to clear the incident.”
- Measure Program Impact—And Use That To Make The Case For Investment. Harvard argues that the goal isn’t simply to collect more data, but to help programs “use existing data systems to generate clear, reliable, and accurate metrics” that allow cities to “compare outcomes and tell compelling stories about their impact.” The toolkit encourages jurisdictions to adopt “a shared data language spoken across jurisdictions” to strengthen “program operations, accountability, and case for investment.” By measuring everything from who is reached to what services are delivered and where additional demand exists, the toolkit gives city leaders a practical framework for demonstrating what’s working—and where programs can continue to grow.
