1. Safer Cities Interview With Medical University Of South Carolina’s Hospital-Based Violence Intervention Program: Turning The Tide. Hospital-based violence intervention programs have become an increasingly important component of the public safety infrastructure in cities across the country. By working to interrupt cycles of violence and reduce the likelihood of future victimization or involvement in violence, healthcare professionals provide medical and trauma services while individuals are hospitalized and help connect survivors to ongoing counseling, legal services, employment support, and educational opportunities.
The Medical University of South Carolina’s Turning the Tide Violence Intervention Program, or TTVIP, serves survivors of violence in Charleston and North Charleston through intensive case management, advocacy, and connections to a wide range of health, social, and community-based services. Safer Cities recently spoke with Ashley Hink, MD, MPH, Trauma Surgeon and Medical Director of TTVIP, about the program’s work, the importance of long-term support, and lessons from serving survivors of violence in Charleston and North Charleston.

- On Why A Team With Lived Experience And Community Connections Delivers Better Outcomes: “The TTVIP client advocates have a variety of lived experiences that help them connect to our patients and families, and importantly they are from the communities where most of our survivors of violence come from in the Charleston and North Charleston areas. Some of the client advocates are survivors of violence themselves or have loved ones who were impacted. Many have work and volunteer experiences in supporting victims of assault, crisis management, mental health services, mentorship, and pastoral care, and are closely tied to other community leaders supporting violence intervention.”
- On The Importance Of Long-Term Support After Injury: “Our program offers and links patients and families to comprehensive services to help with recovery, addressing risk factors for violence, social drivers of health, and to support prosocial development. These include ensuring patients have access to health and rehabilitation services, providing mental health services, transportation to and from appointments, school and employment support, financial support for camps, connections to volunteer opportunities, housing and food access, legal and criminal justice system advocacy and so much more.
Our team follows patients and families for months after injury to ensure they are supported, recovering and thriving. We also have an early intervention program where adolescents and teens who are identified as high-risk for violence in a pediatric primary care clinic get similar comprehensive services.”
- On Building An Effective Violence Intervention Team: “Most people do not realize how intensive the work is, and how comprehensive the services are. Our team members spend incredible time building relationships and trust with patients and families, getting to know their lives, needs and goals. This happens and starts in the healthcare system, then occurs months after injury. They are frequently on phone calls, texts and doing in person meetings within homes and community locations to meet the needs of patients and families. They are truly bridging health care, community care and social care to provide the services that survivors need beyond immediate healthcare needs.
The people that do this work are true professionals and are part of the ecosystem of violence prevention and recovery—their roles are essential for public safety and comprehensive care. Importantly, people don’t always appreciate the emotional intensity of this work, the risk it entails, and the vicarious trauma that team members can experience. They themselves need support, professional development, and outlets for recovery and renewal as they carry a significant burden in supporting survivors of violence.”
2. Report: Roadmap For Using Medicaid To Fund Community Violence Intervention Programs. As states look to expand and sustain community violence intervention efforts, Medicaid is emerging as a promising funding source for both hospital-based and community-based violence intervention initiatives. A new guide published by the Health Alliance for Violence Intervention, or HAVI, outlines how states, counties, healthcare systems, and community organizations can use Medicaid to fund violence prevention services and build long-term sustainability for the field. The report draws on more than a decade of HAVI’s work shaping Medicaid policy and examines the pathways states can use to establish violence prevention benefits, as well as implementation lessons from states that have already done so. As the report explains, its goal is to “equip all violence prevention stakeholders with the knowledge needed to build and sustain Medicaid-funded services for the people at greatest risk of experiencing community violence.” The full report is worth your time, but here are some toplines:
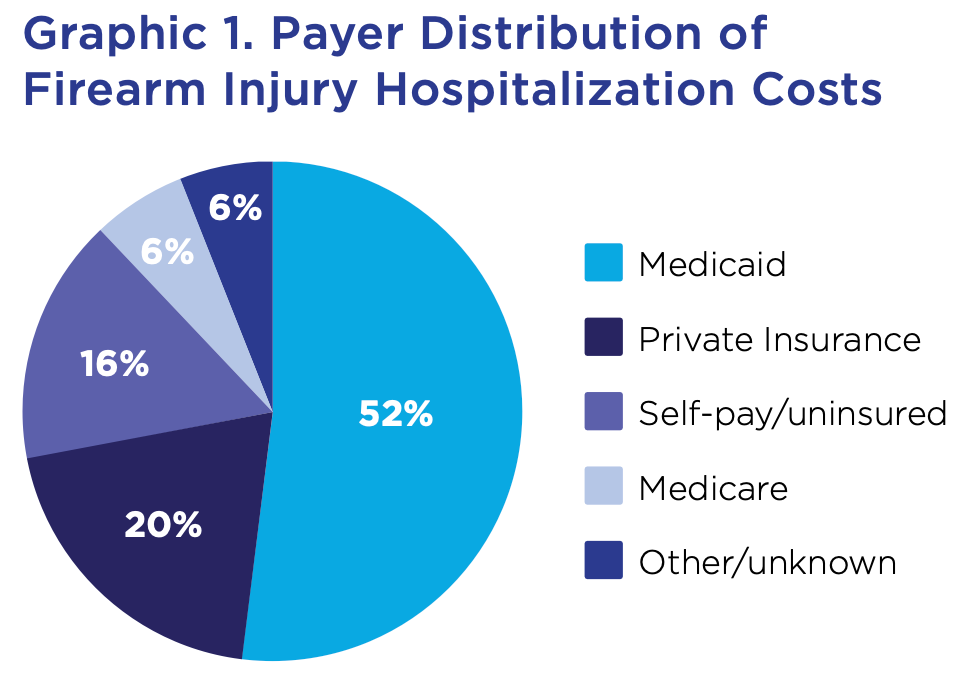
- Medicaid Is A Growing Funding Source For Violence Intervention Programs. Researchers note that “states [are] increasingly turning to Medicaid to support sustainable, evidence-based violence intervention strategies” and argue that “integrating Medicaid policy into public health solutions is crucial to reducing violence and enhancing community safety.” The report also points out that Medicaid already bears much of the financial burden associated with firearm injuries, noting that between 2016 and 2021 firearm injury hospitalizations cost nearly $8 billion, with Medicaid covering approximately $4 billion.
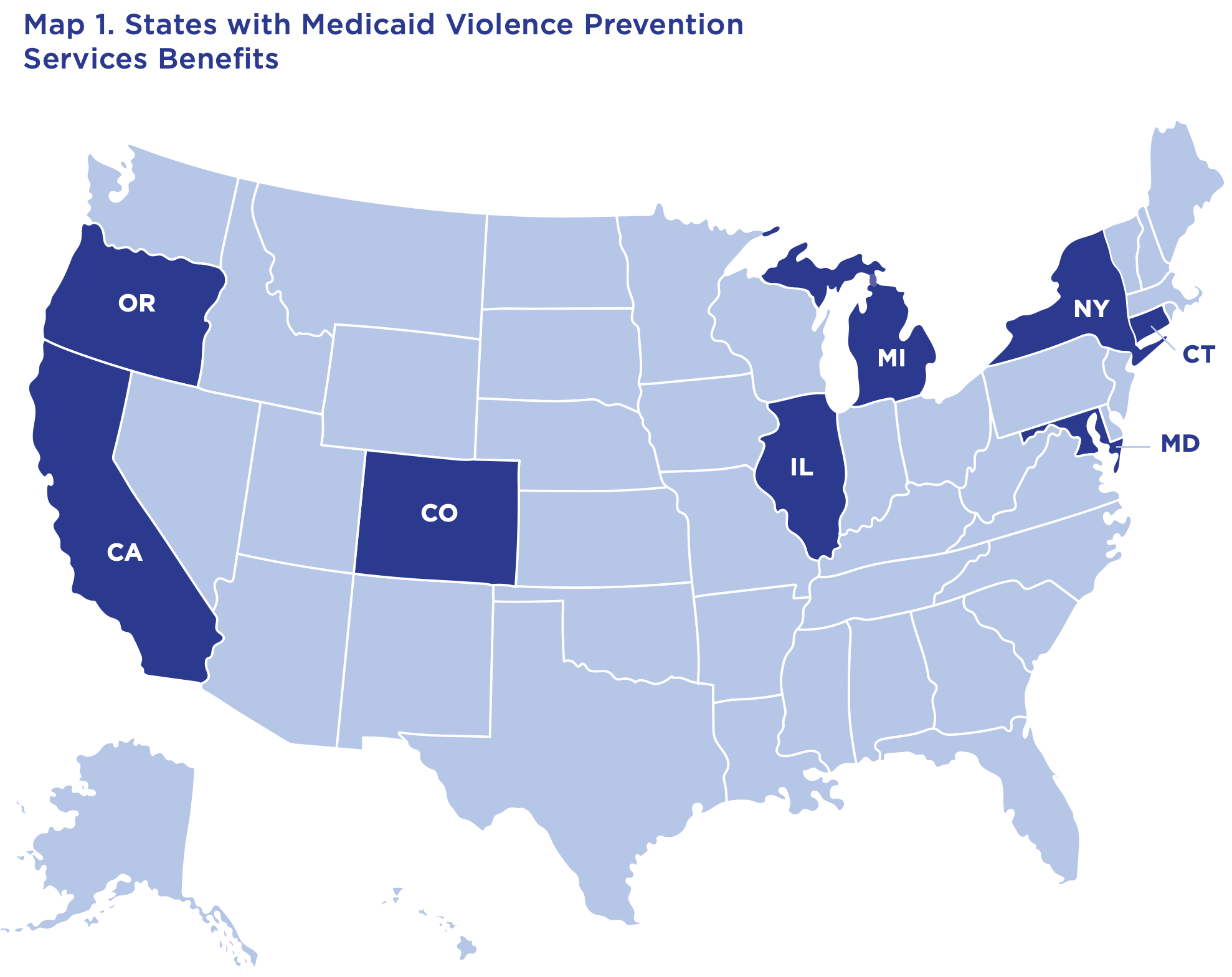
- Eight States Have Already Created Violence Prevention Benefits. According to the report, states can establish violence prevention benefits through “existing mandatory and optional state plan benefits, as well as … other waivers.” In many cases, “a benefit can often be added without passing new legislation if the state Medicaid agency has the authority to create a benefit under existing law,” allowing state officials to establish coverage through the State Plan Amendment process. The report notes that eight states—California, Connecticut, Colorado, Illinois, Maryland, Michigan, New York, and Oregon—have already successfully added violence prevention benefits through legislation, benefit modifications, or state plan amendments.
- The Importance Of Bringing Providers To The Table Early. The report emphasizes that “collaboration is critical for designing a strong and accessible Medicaid violence prevention benefit” and recommends creating a working group that includes “violence prevention experts, Medicaid administrators, health care providers, and community-based organizations.” The group should address practical implementation issues including training and certification standards, billable activities, reimbursement structures, startup funding, and provider billing codes. HAVI also recommends that states recognize multiple certifying organizations to ensure that training aligns with both hospital-based and community-based violence intervention models.
3. Momentum For Hospital-Based Violence Intervention Programs Around The Country.
- In Virginia, Hospital-Based Violence Intervention Program With Reinjury Rate Of “Less Than 2 Percent,” Gets $1.4 Million In Expansion Funding From City. Riverside Regional Medical Center’s Hand in Hand Hospital-Based Violence Intervention Program announced earlier this month that it is expanding following an annual $1.4 million funding commitment from the City of Newport News, which allows the program to operate during “high-volume overnight and weekend hours as well as weekdays.” January Serda, the program’s HVIP Grant Coordinator, said the expansion is important because “in order to break cycles of violence, it’s critical that we do immediate, face-to-face interventions in real time” and “those moments could be our only chance to connect and intervene” to break cycles of violence. The program now encounters “more than 600 victims of intentional violence each year,” and among actively enrolled participants “the rate of reinjury has been very low: less than 2 percent.” Serda said “people at risk of or recovering from firearm injuries often interact with healthcare teams at pivotal moments, so these encounters are critical opportunities for prevention, care and support.”

- In Connecticut, Hospital-Based Violence Intervention Program Provides Direct Cash Assistance To Survivors Of Violence. For The Connecticut Mirror, Emilia Otte reports on an innovative initiative at Yale New Haven Hospital that provides survivors of community violence and intimate partner violence with direct cash assistance. Through the program, victims of violence receive one-time payments of $500, which researchers found helped participants “meet urgent needs, strengthen their connections with community organizations and allow them to take greater charge over their futures.” Dr. Lucy Paredes, a Yale research fellow studying the program, said many survivors faced lost income while recovering from injuries, making financial assistance critical because “when you’re injured and you can’t work, your monthly expenses are coming regardless of what contextual factors are happening.” Researchers found most participants used the funds for “basic necessities” such as “food and rent,” while hospital violence intervention staff said the assistance helps build trust with survivors.

- In Albuquerque, Hospital-Based Violence Intervention Program Reports 307% Increase In Referrals During First Quarter Of 2026. Albuquerque Community Safety’s Hospital-Based Violence Intervention Program reported to Safer Cities that it received 122 referrals during the first quarter of 2026, compared to 30 referrals during the same period in 2025—representing a roughly 307% year-over-year increase. This new data arrives as the city reported receiving 351 referrals last year, compared to 41 referrals the year prior, representing an approximately 756% annual increase. The peer-led program partners with local hospitals to provide “bedside safety planning and ongoing support to victims of violence, traumatic injury, overdose and/or hospitalization,” engaging individuals “at critical points in their recovery” through “peers with lived experience.” Explaining the program’s growth to Safer Cities, ACS Director Jodie Esquibel said: “Our growth is the result of stronger partnerships with hospitals and law enforcement, combined with a more streamlined referral process. Those improvements have allowed our peer support specialists to connect with victims of violence more quickly and consistently during critical moments.”